Improvements in post-surgical mortality for esophageal cancer
Although esophageal cancer remains one of the most deadly cancers, this Swedish population-based study from the Karolinska Institutet documents steady improvement in five-year survival rates over the past two decades. Among 2,291 patients undergoing esophageal cancer surgery, survival increased by about 3% per year despite patients being older and having more advanced tumors and comorbidities over time. The decrease in mortality hazard ratios reflects advancements in preoperative imaging, neoadjuvant therapies, surgical techniques, and perioperative care. These survival gains were particularly notable among patients with higher comorbidity scores and were not solely attributable to changes in surgery rates or patient selection, indicating overall progress in treatment strategies and centralization of care.
Time Trends in Survival After Surgery for Esophageal Cancer in a National Population-Based Study in Sweden.
Lundberg E, Mattsson F, Gottlieb-Vedi E, Lagergren J.
Abstract
Background: The long-term survival after surgery for esophageal cancer has improved over the past few decades, but studies that assess recent survival trends are lacking.
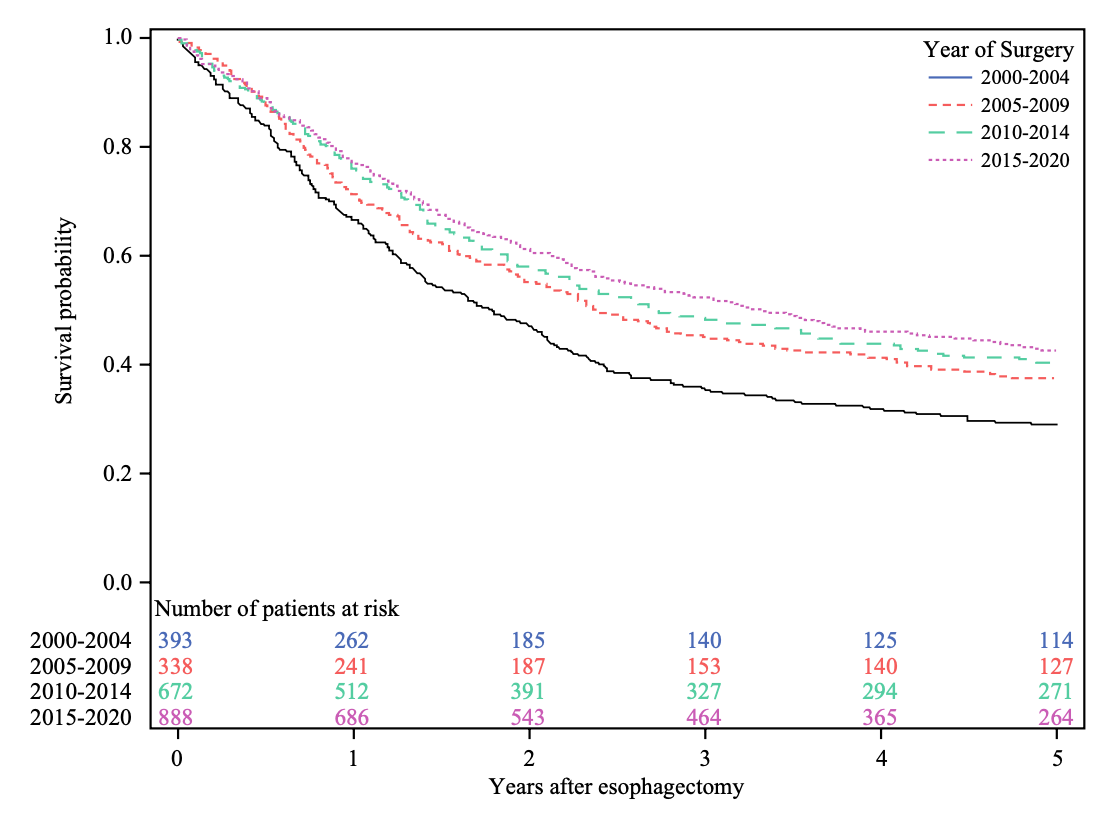
Methods: This population-based cohort study included 2291 patients who underwent esophagectomy for esophageal cancer in Sweden between 2000 and 2020, with follow-up until 2024. Data came from medical records and national registries. Calendar time was analyzed as a continuous and categorized variable. The main outcome was all-cause 5-year mortality. Secondary outcomes were disease-specific 5-year mortality and 1-year all-cause mortality. Multivariable Cox regression provided hazard ratios (HR) with 95% confidence intervals (CI), adjusted for age, sex, comorbidity, tumor histology, neoadjuvant therapy, hospital volume, and pathological tumor stage.
Results: The study period witnessed increasing resection rates, centralization to fewer hospitals, and improving postoperative 5-year survival. When analyzing calendar time as a continuous variable, the adjusted HR for all-cause 5-year mortality was 0.97 (95% CI 0.95-0.98). In categorized analyses, the HRs decreased for each later time period and was 0.57 (95% CI 0.47-0.69) comparing the surgery period 2015-2020 with 2000-2004. The trends were similar for disease-specific 5-year mortality and all-cause 1-year mortality. In stratified analyses, patients with Charlson comorbidity score ≥2 had the strongest improvement in all-cause 5-year mortality (HR 0.45, 95% CI 0.30-0.69 comparing surgery in 2015-2020 with 2000-2004).
Conclusions: The recent 5-year survival has improved after surgery for esophageal cancer in Sweden. This improvement is not explained by lower surgery rates or selection of surgical candidates of younger age, fewer comorbidities, or earlier tumor stage.