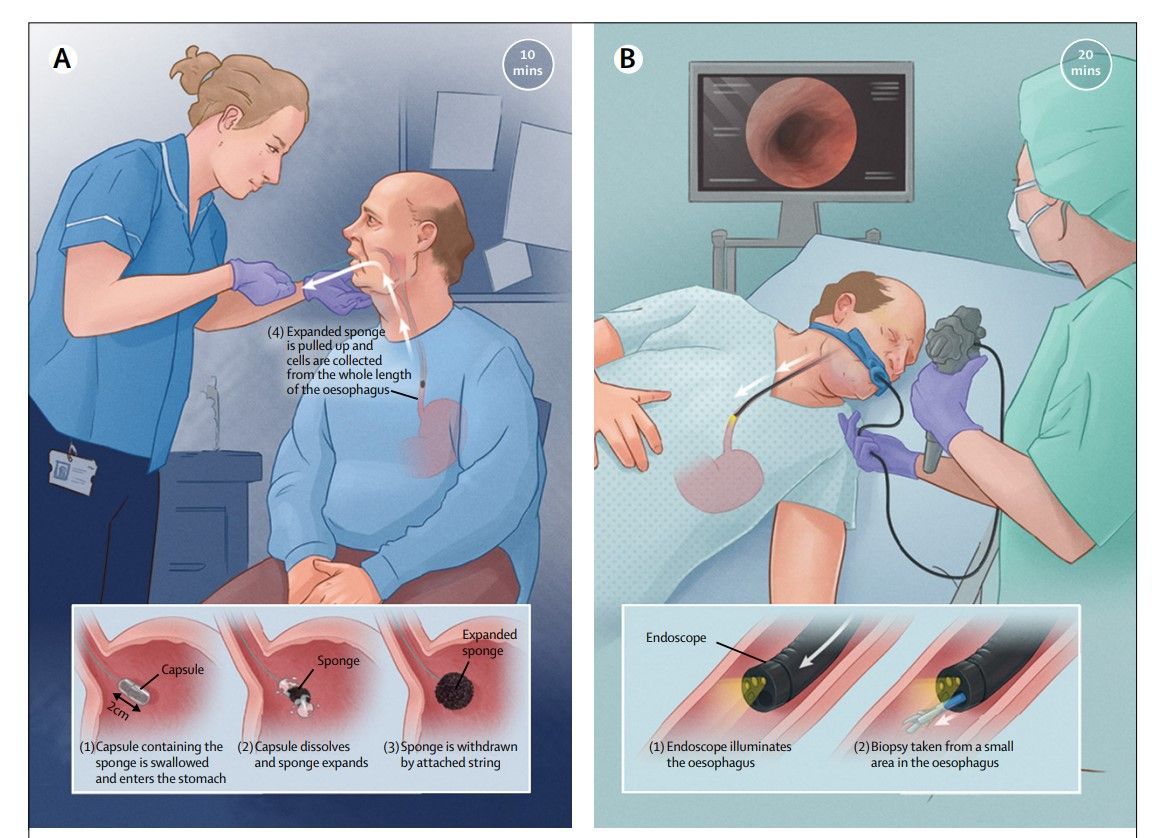
Utility of cytosponge demonstrated
This impressive randomized trial observed an approximately 10-fold increase in detection of Barrett's with use of the Cytosponge non-endoscopic test. Nine persons in the Cytosponge group were found to have treatable dysplasia or early stage cancer vs. none in the usual care group.
Lancet. 2020 Aug 1;396(10247):333-344.
doi: 10.1016/S0140-6736(20)31099-0.
Cytosponge-trefoil factor 3 versus usual care to identify Barrett's oesophagus in a primary care setting: a multicentre, pragmatic, randomised controlled trial
Rebecca C Fitzgerald 1 , Massimiliano di Pietro 2 , Maria O'Donovan 2 , Roberta Maroni 3 , Beth Muldrew 3 , Irene Debiram-Beecham 4 , Marcel Gehrung 5 , Judith Offman 6 , Monika Tripathi 2 , Samuel G Smith 7 , Benoit Aigret 3 , Fiona M Walter 8 , Greg Rubin 9 , BEST3 Trial team; Peter Sasieni 3
PMID: 32738955 PMCID: PMC7408501 DOI: 10.1016/S0140-6736(20)31099-0
Free PMC article
Abstract
Background: Treatment of dysplastic Barrett's oesophagus prevents progression to adenocarcinoma; however, the optimal diagnostic strategy for Barrett's oesophagus is unclear. The Cytosponge-trefoil factor 3 (TFF3) is a non-endoscopic test for Barrett's oesophagus. The aim of this study was to investigate whether offering this test to patients on medication for gastro-oesophageal reflux would increase the detection of Barrett's oesophagus compared with standard management.
Methods: This multicentre, pragmatic, randomised controlled trial was done in 109 socio-demographically diverse general practice clinics in England. Randomisation was done both at the general practice clinic level (cluster randomisation) and at the individual patient level, and the results for each type of randomisation were analysed separately before being combined. Patients were eligible if they were aged 50 years or older, had been taking acid-suppressants for symptoms of gastro-oesophageal reflux for more than 6 months, and had not undergone an endoscopy procedure within the past 5 years. General practice clinics were selected by the local clinical research network and invited to participate in the trial. For cluster randomisation, clinics were randomly assigned (1:1) by the trial statistician using a computer-generated randomisation sequence; for individual patient-level randomisation, patients were randomly assigned (1:1) by the general practice clinics using a centrally prepared computer-generated randomisation sequence. After randomisation, participants received either standard management of gastro-oesophageal reflux (usual care group), in which participants only received an endoscopy if required by their general practitioner, or usual care plus an offer of the Cytosponge-TFF3 procedure, with a subsequent endoscopy if the procedure identified TFF3-positive cells (intervention group). The primary outcome was the diagnosis of Barrett's oesophagus at 12 months after enrolment, expressed as a rate per 1000 person-years, in all participants in the intervention group (regardless of whether they had accepted the offer of the Cytosponge-TFF3 procedure) compared with all participants in the usual care group. Analyses were intention-to-treat. The trial is registered with the ISRCTN registry, ISRCTN68382401, and is completed.
Findings: Between March 20, 2017, and March 21, 2019, 113 general practice clinics were enrolled, but four clinics dropped out shortly after randomisation. Using an automated search of the electronic prescribing records of the remaining 109 clinics, we identified 13 657 eligible patients who were sent an introductory letter with 14 days to opt out. 13 514 of these patients were randomly assigned (per practice or at the individual patient level) to the usual care group (n=6531) or the intervention group (n=6983). Following randomisation, 149 (2%) of 6983 participants in the intervention group and 143 (2%) of 6531 participants in the usual care group, on further scrutiny, did not meet all eligibility criteria or withdrew from the study. Of the remaining 6834 participants in the intervention group, 2679 (39%) expressed an interest in undergoing the Cytosponge-TFF3 procedure. Of these, 1750 (65%) met all of the eligibility criteria on telephone screening and underwent the procedure. Most of these participants (1654 [95%]; median age 69 years) swallowed the Cytosponge successfully and produced a sample. 231 (3%) of 6834 participants had a positive Cytosponge-TFF3 result and were referred for an endoscopy. Patients who declined the offer of the Cytosponge-TFF3 procedure and all participants in the usual care group only had an endoscopy if deemed necessary by their general practitioner. During an average of 12 months of follow-up, 140 (2%) of 6834 participants in the intervention group and 13 (
Interpretation: In patients with gastro-oesophageal reflux, the offer of Cytosponge-TFF3 testing results in improved detection of Barrett's oesophagus. Cytosponge-TFF3 testing could also lead to the diagnosis of treatable dysplasia and early cancer. This strategy will lead to additional endoscopies with some false positive results.