Predicting risk of esophageal adenocarcinoma
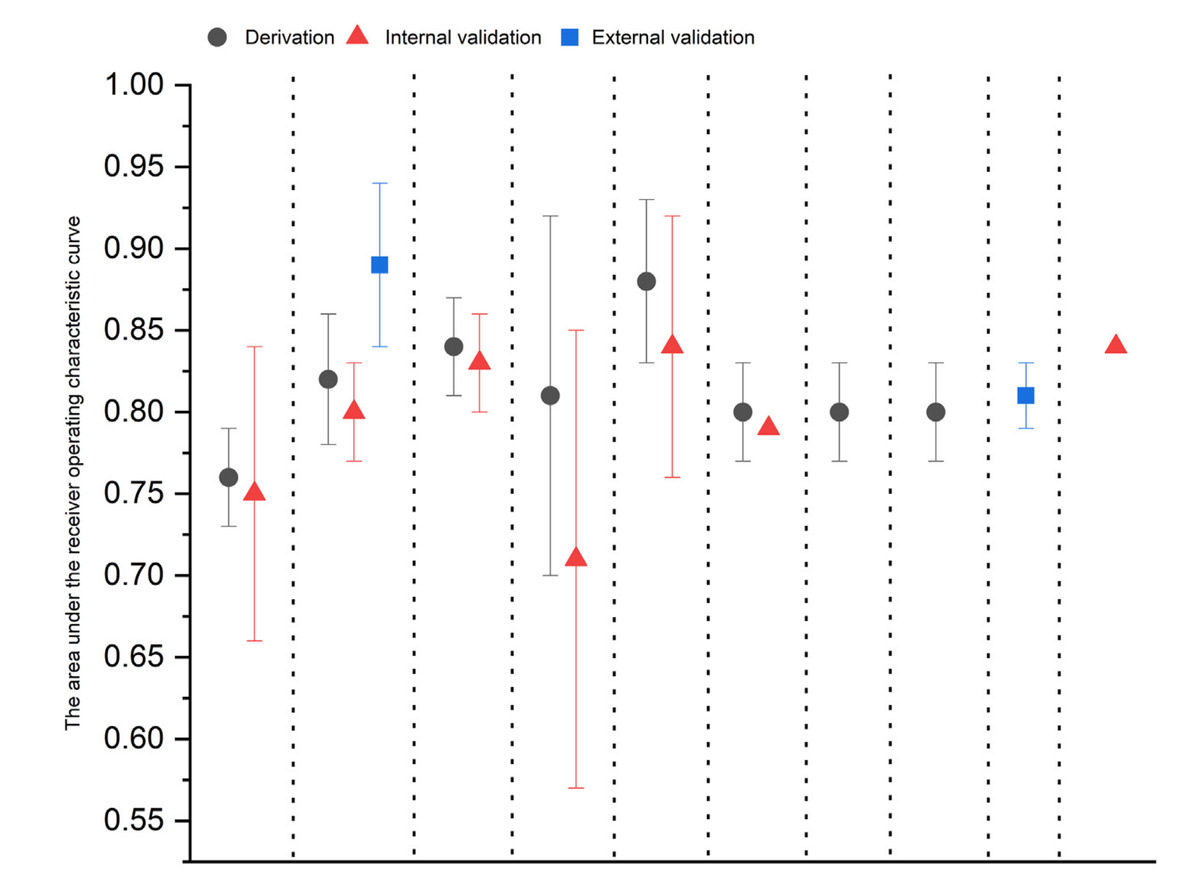
This systematic review from investigators at the Karolinska Institute and Fujian Medical University evaluates nine risk prediction models from seven studies aimed at identifying individuals at high risk for esophageal adenocarcinoma (EAC) to improve targeted screening and early detection. The models commonly use predictors such as age, sex, GERD symptoms, BMI, and smoking status, with some incorporating the presence of Barrett's esophagus, family history, polygenic risk scores and potential protective factors such as aspirin, statins and physical activity. While these models demonstrate good discriminative ability (AUC 0.76–0.88) and calibration in cohort studies, all suffer from high risk of bias, mainly due to data analysis issues like inadequate handling of missing data and potential overfitting. Most models lack external validation, limiting their clinical applicability. The review highlights challenges including the low absolute risk even in high-risk groups, the exclusion of Barrett’s esophagus as a predictor, and the need for cost-effectiveness analyses. The authors recommend further external validation, methodological improvements, and careful determination of risk thresholds before these models can be widely implemented.
A Systematic Review of Risk Prediction Models for Esophageal Adenocarcinoma in the General Population.
Zhao L, Chen B, Lagergren J, Xie SH.
Abstract
BACKGROUND AND AIMS: Risk prediction models can identify individuals at high risk of esophageal adenocarcinoma. This systematic review aimed to critically appraise the available models for projecting absolute risk of esophageal adenocarcinoma in the general population. METHODS: We searched Medline, Embase, and Cochrane Library databases for studies of risk prediction models for esophageal adenocarcinoma. Data were extracted from eligible studies according to the checklist for critical appraisal and data extraction for systematic reviews of prediction modelling studies. Risk of bias and applicability were assessed using the prediction model risk of bias assessment tool. RESULTS: We identified 7 studies. Age, sex, gastroesophageal reflux disease, body mass index, and tobacco smoking were the most common predictors. The area under the receiver operating characteristic curve ranged between 0.76 and 0.88 in the derivation datasets. The models based on 2 cohort studies showed good agreement between observed and predicted risks. All studies had at least 1 domain with high risk of bias, primarily attributable to methodological shortcomings in the data analysis. CONCLUSION: Most risk prediction models showed good performance in identifying individuals at high risk of esophageal adenocarcinoma. Validation in external populations and cost-effectiveness evaluation are needed before these models can be applied in public health and clinical practice.